Why You Can Buy Medicine in Bulk in the U.S. — but Not in Ireland

Ireland’s pharmacy rules reflect a broader European approach that prioritizes control over access — with consequences for how patients buy and use medicine.
DUBLIN, IRELAND (March 19, 2026) — When friends in the United States ask what they should bring on a trip to Ireland, the advice is not what they expect.
Bring your own medication.
It is not the kind of tip that shows up on travel websites, but it is one I give consistently. Americans are used to walking into a store and buying what they need — whether it is a bottle of Tylenol, Aleve or something to help with sleep after a long flight.
In Ireland, and across much of Europe, it is not always that simple.
Travelers who assume they can replace what they run out of often find smaller pack sizes, higher prices and, in some cases, the need to speak with a pharmacist before making a purchase. The experience can be surprising enough that many later say they wish they had known in advance.
The advice tends to be appreciated because it is not obvious. While most common medications are available in Ireland, access is more restricted and less convenient than in the United States.
What makes the system more confusing for Americans is that the rules are not always intuitive. Some medications that are tightly controlled in the United States are easier to obtain in Ireland, while others are far more restricted. Low-dose Codeine combination products, for example, are available over the counter in Ireland with pharmacist supervision, while in the United States they require a prescription. At the same time, Melatonin — widely sold in bulk as a supplement in the United States — is generally treated as a medicine in Ireland and is typically available only by prescription. The result can feel contradictory to American visitors, but reflects a different regulatory logic: controlling how drugs are used, rather than simply how they are classified.
For that reason, I tell people to bring whatever they expect to need rather than rely on buying it here.
The difference is not the drugs. It is the system.
While this experience is framed through Ireland, the same rules and philosophy apply across much of the European Union, where medication access is more tightly controlled than in the United States.
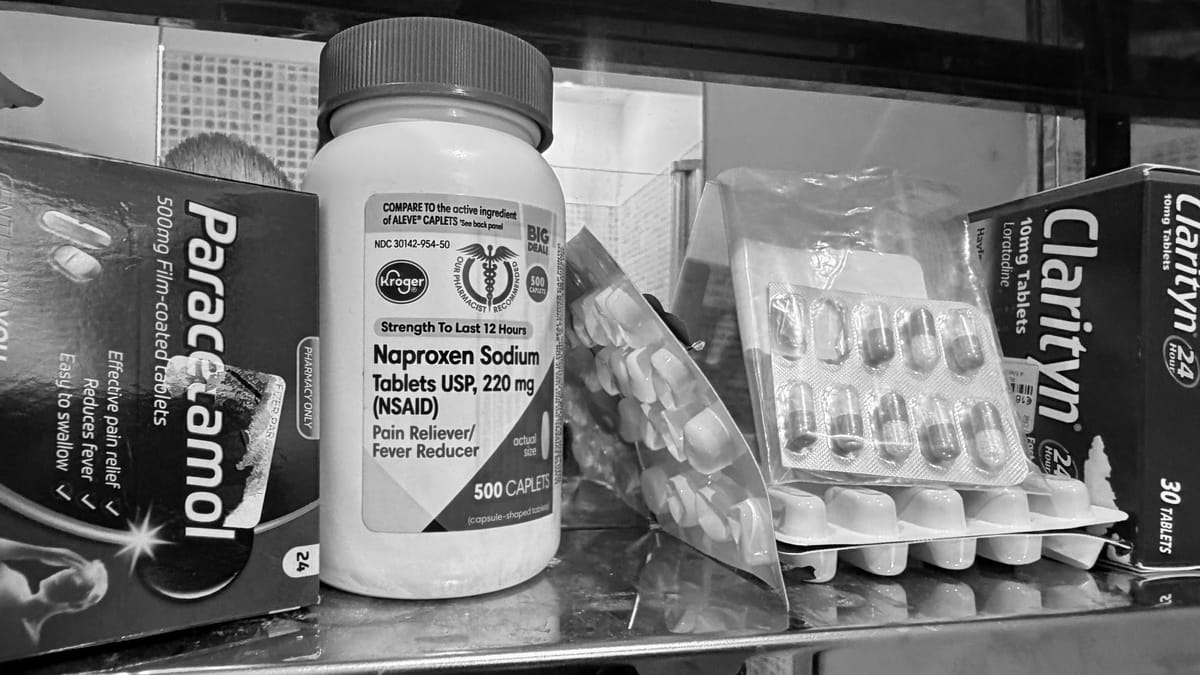
Across everything from Paracetamol — known in the United States as acetaminophen — to Melatonin, the United States and Ireland take fundamentally different approaches to who controls access to medication: patients or the healthcare system.
Bulk Access vs Controlled Access at the Pharmacy Counter
In the United States, most over-the-counter medications are sold in bulk with minimal oversight. Consumers can purchase large quantities without interacting with a pharmacist, driving down the price per pill and maximizing convenience.
In Ireland and much of the European Union, many of the same medications are subject to pack-size limits and pharmacist supervision. Some are classified as “pharmacy-only,” meaning they do not require a prescription but cannot be freely taken off the shelf. Others require a prescription, which can add an additional layer of cost and inconvenience. A visit to a general practitioner can cost €60 or more, and it is not always simple to find a doctor or secure a convenient appointment, particularly for visitors.
Melatonin highlights the divide. In the United States, it is widely sold as a dietary supplement in bottles of 100 to 300 tablets or gummies. In Ireland and across much of Europe, it is generally treated as a medicine and is typically available only by prescription or under limited conditions.
The policy logic is clear: smaller quantities and pharmacist oversight are intended to reduce overdose risk, misuse and long-term dependence.
Pain Management: A Different Kind of Control
The same philosophy appears in clinical care.
After suffering a broken leg in Ireland, I was treated with morphine and then prescribed OxyContin for pain.
Concerned about the risk of dependence, I asked to come off the opioid and switch to something less potent — what in the United States would often be a “middle” option such as a hydrocodone combination product.
Instead, I was offered Paracetamol (i.e., Tylenol) typically used for mild to moderate pain and fever.
When I pushed to step down, my doctor advised against it, saying I was coming off the opioid too early and should remain on it longer to properly manage the pain.
The choice was effectively binary: continue with a strong opioid or transition to non-opioid treatment, often combined with anti-inflammatory drugs.
What was missing was a familiar middle ground — a reflection of a broader European reluctance to rely on intermediate opioid prescribing.
One System, Two Outcomes
These two experiences — one at the pharmacy counter and one in a hospital — reflect the same underlying approach.
In Ireland and much of Europe, access to medication is controlled at the front end. That includes limiting quantities, requiring pharmacist involvement and, in some cases, avoiding intermediate opioid prescribing.
In the United States, the system has historically emphasized access and consumer autonomy, allowing bulk purchasing and offering a wider range of step-down options in pain management.
Each model solves one problem by creating another.
Ireland’s approach may reduce misuse and long-term dependence but can introduce friction for patients and, at times, more abrupt transitions in care.
The American system offers convenience and flexibility, including smoother step-down pathways, but has also contributed to higher rates of overuse and, in the case of opioids, significant public health consequences.
A Question of Who Decides
The medications themselves are largely the same.
The difference lies in who is trusted to decide how they are used — the patient standing at the counter, or the system designed to guide and, when necessary, limit that choice.
This article was prepared with the assistance of AI tools under the direction and editing of Robert Cox.